Orofacial Myofunctional Disorders (OMD’s)
What Are OMD’s?
Disorders in the working muscles of the face, including the tongue, lips, and jaw, can result in an incorrect swallowing pattern, and/or an abnormal open mouth resting posture. OMD’s can result from a series of causes including digit (thumb, finger) sucking, tethered oral tissues (TOT’s), extended pacifier and bottle use, nail biting, or Trichotillomania (hair pulling, skin picking) habits, tethered oral tissues (TOT’s), and/or nasal airway blockage. The open mouth resting posture, along with nasal airway obstruction(s) can often lead to a retained “mouth breathing” habit.
Chronic mouth breathing can lead to changes in growth, development and/or neuromuscular dysfunctions. OMD’s may affect-directly or indirectly- breastfeeding, facial skeletal growth and development, chewing, swallowing, speech, dental occlusion, temporomandibular joint movement, oral hygiene, periodontal health, stability of orthodontic treatment, facial esthetics, and sleep postures.
Low tongue posture, tongue tie and parafunctional habits are precursors to tongue thrust. A normal swallow involves the tongue tip elevating to the spot (incisive papilla), a palatal front cave suction to the anterior portion of the palate, followed by the back of the tongue rising and sealing the hard palate, creating what is called the peristaltic wave. The lifting of the posterior tongue to seal the soft palate creates a negative pressure and lets the epiglottis completely cover the trachea and the esophagus to open without force for a safe swallow.
The registered dental hygienist can be the dental allied leader in recognizing dysfunctional patterns in airway, and in its resulting impact on craniofacial and dental development during preventive care appointments. Some dental hygienists choose to specialize in the field of orofacial myofunctional therapy with additional training and certification. The primary role of OMT is to establish a tongue in the palate oral rest and swallowing posture, a closed lips resting posture, with a patent nasal airway. The steps involved in establishing this include many variables.
What causes OMD’s?
Mouth Breathing vs Nasal BreathingWe are born nasal breathers, but if something occurs to clog the nasal passages, or perhaps a posterior tongue tie exists holding the tongue down, or one develops a sucking habit, then we begin to utilize the open mouth posture for breathing. This change in the lower jaw and tongue position leads to an elongated face and narrow upper palate often referred to as “long face syndrome”. A low, forward tongue and jaw posture leads to a forward head and neck posture, a collapsed chest and airway, and associated toes walking. Mouth breathing can stimulate the vagus nerve, which regulates breathing and digestion, and can elicit anxiety.
Read More

Characteristics of open mouth posture include:
- Open, dry lips
- Short upper lip, gummy smile
- Recessed, dimpled (golf ball) chin
- Dark circles under the eyes (shiners)
- Nasal salute line across the middle of the nose
- Dental gingivitis and decay issues
- Narrow upper/maxillary palate
- Teeth crowding
Nearly 90% of mid-face growth occurs from birth to age 7. The vertical elevation of the tongue (including the posterior seal) is necessary for the optimal development of the maxilla palate and stimulation of the palatal structures for growth.
The development of the nasal cavity depends on the development of the palate. Patent nasal passages, along with elevation of the tongue in the oral cavity are key to the lasting reeducation of breathing, and mandatory for eliminating mouth breathing. Obstructions such as enlarged tonsils, swollen nasal turbinates, or a deviated nasal septum may necessitate a referral to an ENT or allergist to assist in achieving a patent nasal airway. Evaluation and treatment by a functional dentist or orthodontist are indicated with the presence of a high, narrow palate.
The benefits of a patent nasal airway and nasal breathing:
- Nasal passages warm and humidify the air and provide the antibacterial benefits of nitric oxide, which in turn helps to increase the uptake of oxygen into the lungs and distributes more oxygen throughout the body.
- Slow, nasal breathing is essential for good mental health, a parasympathetic (rest and digest) state of calmness.
- Mouth breathing results in a chronic sympathetic state of “fight or flight.”
- Nasal breathing is important in assisting with many airway issues such as sleep disordered breathing (SDB) and obstructive sleep apnea (OSA).
- Sleep and breathing are linked, and sleep disordered breathing (SDB) effects psychological and emotional development of a growing child.
FAQ

What Can Orofacial Myofunctional Therapy (OMT) Accomplish?
- Normalize tongue and lip resting postures
- Establish nasal breathing patterns
- Eliminate improper chewing and swallowing patterns
- Stabilize the dentition from extraneous orofacial muscle movement
What Age Should You Start?
Children from birth can benefit from an evaluation to determine if causal factors such as the inability to breathe from their nose consistently, or if a tongue/lip tie(s) requires intervention. If so, they can receive the appropriate referrals to other specialty professionals for optimum growth and development.
Children as young as three to five years of age can begin a program (digit sucking, etc.) to help eliminate harmful sucking habits that. without therapy and the addition of a “mini-myo program”, may result in orofacial myofunctional disorders.
Children from birth to seven years of age are good candidates for the correction of early dysfunctions (OMD’s) through orofacial myofunctional therapy.
Teens and adults of all ages are also able to achieve successful, long-term results.
What Are Harmful Habits That Need To Be Addressed?
- Prolonged pacifier use
- Thumb and/or finger sucking
- Fingernail, cheek, or lip biting
- Tongue sucking
- Clenching or grinding of the teeth
How Does OMT Benefit Patients?
- Aiding in the development of normal patterns of dental eruption and alignment
- Assisting in the stabilization of the teeth during and/or after orthodontic treatment or jaw surgery
- Identifying the need, and supporting the remediation of speaking errors – different than some traditional speech therapy methods
8 Step Checklist
- Does or did your child use a pacifier, have a digit, tongue sucking or nail-biting habit?
- Is there nasal congestion, food and/or seasonal allergies present?
- Are the lips parted, the tongue resting low or extending between the teeth and lips?
- Are or was your child a messy or noisy eater?
- Do or did your child drool during daytime hours or while sleeping?
- Is there any restriction in the movement of the tongue or lips?
- Are or was your child slow in speaking, and/or their speech mumbled or garbled?
- Are or was your child a restless sleeper, or do they snore/experience noisy breathing?
If you answered yes to any of the above questions, your child may benefit from a consultation to assist your child in becoming their best self.
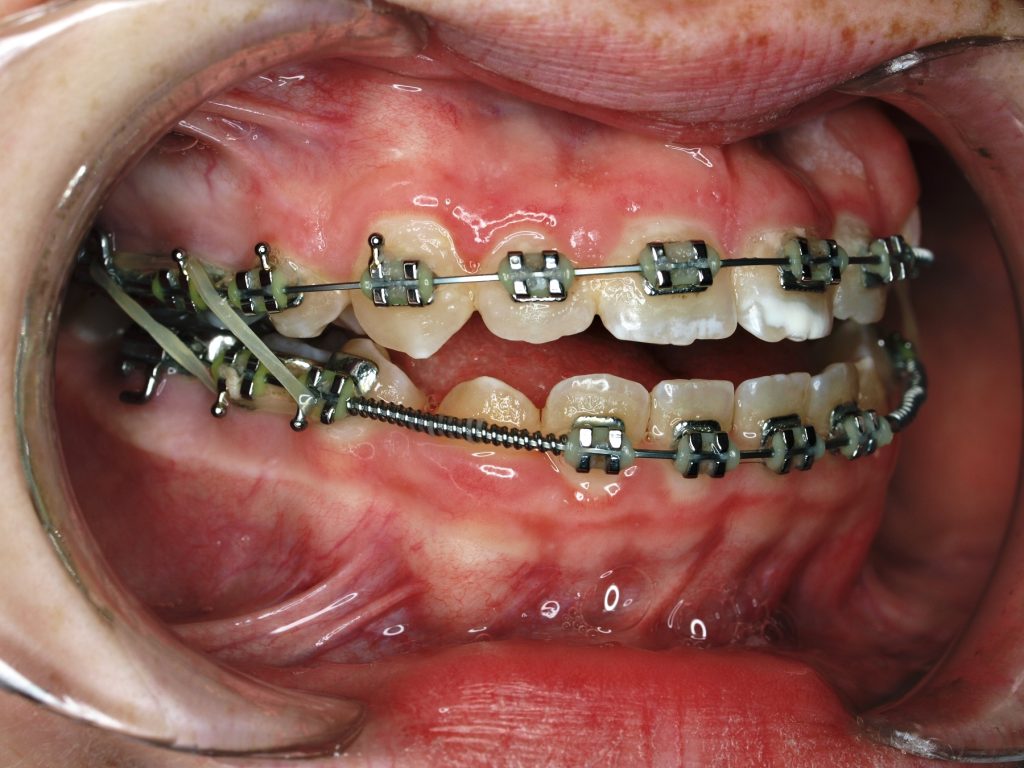
Tongue Thrust
Normal oral resting posture includes lips lightly pressed together, teeth slightly apart, tongue resting in the roof of the mouth with tip on “spot”, and breathing through the nose. But, when a person swallows incorrectly, the tongue often presses against or spreads between the teeth and/or rests low in the mouth. This is commonly referred to as a “tongue thrust”. Retained in a forward posture, the anterior portion of the tongue often extends past the front teeth while eating, chewing, or swallowing and speaking.Read More
A dysfunctional swallowing pattern is caused from an insufficient backward pull of the tongue. The chin and lip muscles tighten to help facilitate the gathering of saliva, instead of the posterior muscles of the face and tongue participating in the swallowing process-allowing air to be swallowed.

Constant thrusting of the tongue between the teeth can prevent normal teeth eruption, can push existing teeth out of place and cause dental malocclusions including anterior, unilateral, and bilateral open bites, and/or dental crossbite(s). When the tongue extends against or past the front teeth with chewing it can cause an anterior overjet (protruding upper front teeth) and/or create a dental Cl II or Cl III malocclusion. A retained low tongue posture can cause the palate to become high and narrow, and the nasal airway (sinus cavities) to become small and compromised. If not corrected, growth and development adaptations can lead to post orthodontic treatment relapses. When speaking, a low tongue posture can result in a condition commonly referred to as a “lisp”.
Speaking Disorders
Speech is how air is impacted by muscle movement. It involves abdominal and velum grading and activity of the oral structures of the tongue, lips, and jaw. Weak muscle tone can prevent the proper development of oral motor skills needed for correct articulation and production of speech. Some symptoms of speech impairments can include the muscles of the cheeks, chin and lips forming a “facial grimace”.Read More

Speaking disorders can reduce a person’s ability and willingness to communicate audibly, and may result in a reliance on gestures, sign language, and/or other forms of communication. The myofunctional therapist works with patients to define dental proprioception and sensory awareness of oral movements, and to develop supportive muscle tone and correct swallow patterns.
Tethered Oral Tissues
Initially the tongue and the floor of the mouth develop as one, but as an embryo grows, the tongue separates from the floor of the mouth. When this does not occur in proper form, it results in a “tongue-tie”. Tethered oral tissues (TOT’s) can affect the fascial tissues from the top of the head to the tip of the toes, and often results in tension of the muscles of the head, neck, shoulders, and beyond.Read More
Not all medical and dental providers are trained in the most current systems used to recognize the functional limitation of tethered oral tissues (TOT’s) including lip, buccal (cheek) and tongue ties. Often the anterior portion of the tongue appears normal, but the posterior position is overlooked. Doctors Guilleminault, Ghaheri, Kutlow, Zaghi and Baxter have led the way with their research in understanding the fascial dynamics involved by restrictions, and in creating a protocol for the identification and treatment of ties.

Comprehensive TOT’s treatment combines the services of an International Board-Certified Lactation Consultant (IBCLC), myofunctional therapist (OMT), chiropractor/osteopath, and/or craniosacral therapist (CST) prior to release. There are times when the combination of these specialist’s treatment(s) can incorporate the supporting structures and/or fascia, and thus reduce the need for tie release(s). There are also times when a tongue tie attachment extends to the physical tongue tip (Class III, or IV) and/or the posterior regions of the tongue, “posterior insertion”, may warrant release. An infant CL III or IV upper lip tie may need to be released to allow for proper suck/swallow form. Tethered oral tissues are genetically predisposed, and often go undetected and/or undiagnosed without help from this specialty team.
In infants the myofunctional therapist plays a vital role in assisting infants by incorporating intraoral stimulation of the mouth and guiding correct form and function-with parent participation. Infant tie involvement symptoms related to breastfeeding include:
- Inability to latch to the breast
- Digestive issues: fussy, gassy, colicky
- Nursing often, spitting up, falling asleep
- Failure to thrive
- Mother: pain, mastitis, lack of production of ample milk supply


In children, myofunctional therapy can set the stage for a successful release when the child is developmentally ready. In general, a young child needs to be old enough to do the three C’s:
- Comprehend the exercises
- Cooperate with therapy
- Comply with pre and post operative care
Many adults suffer from the consequences of the long-term restrictions of tethered tissues if not treated, as they are unaware of the cause of the problems and associated postural restrictions and/or pain.
Kathleen, as an experienced Certified Orofacial Myologist (COM) can complete a comprehensive evaluation, provide appropriate therapy, and work closely with the doctors who perform the actual release procedure(s).
Breathing Disorders
There is a direct relationship between airway, proper nasal breathing, and facial growth development. The only time our mouths should be open besides the intake of food and drink, speaking, or cleaning one’s mouth is by default, due to nasal blockage. A low, forward tongue posture brought on by habitual mouth breathing can lead to long term structural compromises including enlarged tonsils/adenoidal tissues, narrow palate, narrow sinus cavities and/or resulting deviated septum.Read More
Any disruption in normal breathing form and function reduces nasal airway exchange. Any altered mechanics can lead to reduced nitric oxide and lower carbon dioxide levels in the blood stream.
Mouth breathing results in a chronic sympathetic state of “fight or flight”. If sleep is altered the entire psychological emotional development of a growing child is influenced. Nasal breathing is important in assisting with many airway issues such as sleep disordered breathing (SDB) and obstructive sleep apnea (OSA).
A CBCT (3-D scan) used in dentistry is the most comprehensive means of evaluating for airway obstructions (and/or the presence of temporomandibular joint disorders). An Otolaryngologist or Ears, Nose, and Throat (ENT) specialist can determine if there are any structural causes(s) for forward resting tongue posture due to nasal airway obstruction(s) using a lighted scope during an examination.
Through a multidisciplinary approach, sleep specialists are working with myofunctional therapists to further control sleep disorders. Treatment emphasizes proper oral posturing and silent nasal breathing. A patent nasal airway can have a dramatic effect on one’s ability to function in everyday life, on physical appearance, and overall long-term health.
Testimonial
“The left corner of my lip drooped downward for many years. While this was emotionally upsetting, I wasn’t aware of any professional that could help my lips look normal again. After seeing Kathleen help my grandson with his tongue tie, I learned about orofacial myology. Kathleen is a leader in this field and has many more years of experience than many in this field.
The help Kathleen provides has increased my confidence and I’m so thankful for her expertise.”
– Jean
Jaw Pains And Headaches

The tongue and facial muscles play a crucial role in stabilizing the jaw. Over time, neuromuscular dysfunctions can cause the lower jaw to become unstable, often resulting in intense jaw pain and headaches. This instability of the jaw can lead to temporal mandibular disorders (TMJ). The National Institutes of Health (NIH) defines temporomandibular joint (TMJ) disorders as:
- Discomfort or pain in the muscles that control jaw function
- A displaced disc, dislocated jaw, or injury to the condyle
- Degenerative/Inflammatory joints
Digestive Disorders

Digestive issues and orofacial myofunctional disorders are connected. Digestion starts in the mouth. Digestive issues can occur for many reasons:
- Lack of sensory perception of food in the mouth – results in stuffing the mouth
- Poor development of the masseters and muscles of mastication for chewing-resulting in poor chewing of food items
- Less digestive enzymes dispensed intraorally
- Drinking an increase in liquids to wash down food-resulting in choking on solids, stomach aches, and/or constipation
50% of the lymphatic system is in the gut. Lymphatic health is intertwined with the health of our entire body. To get the most out of meals, try to cultivate these habits:
- Avoid technology, as the electric and magnetic fields (EMFs) will make it harder for the body to get into parasympathetic rest and digest mode.
- Avoid drinking cold beverages while eating, as it slows digestion and dilutes stomach acid needed to properly break down food.
- Chew food well, as it helps to mix food with enzyme rich saliva.